Clinical Assessment of Jaw Position

During the physical examination, one determines the position of the maxilla and mandible in three-dimensional space. This is done separately for each facial axis: anteroposterior, vertical, and transverse.
Anteroposterior
One infers the anteroposterior position of the jaws by evaluating the anteroposterior occlusal relationships and the facial profile. The occlusal relationships are appraised at three different sites: first molar, canine, and central incisor (Figure 3). With this appraisal, the frame of reference is the upper dentition and the examiner gauges the anteroposterior position of the lower teeth in relation to a hypothetical static upper.
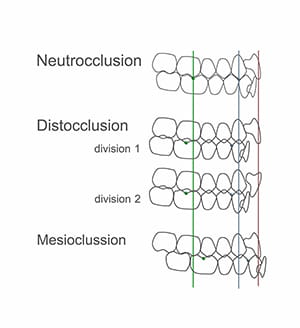
Figure 4
Angle’s classifications of molar relationship assesses the position of the buccal groove of the lower first molar in relation to the mesiobuccal cusp of the upper.13 In an ideal Class I molar relationship, these landmarks coincide (i.e., align). In a Class II relationship, the lower molar groove is behind the upper cusp; whereas, in a Class III, it is in front. The canine region is assessed in a similar manner. In a Class I canine relationship, the lower-canine-first-premolar embrasure coincides with the cusp of the upper canine. In a Class II, the embrasure is behind the upper canine cusp; with a Class III, it is in front.
Finally, for the incisal region, we measure the overjet, which is defined as the horizontal distance between the incisal edges of the upper and lower central incisors. When the lower incisal edge coincides with the upper, the overjet is zero. When it is behind, the measurement has a positive value; when in front, it will be negative. The ideal overjet is +2mm.
Based on the above referenced assessments, one classifies the occlusion into neutrocclusion, distocclusion, or mesiocclusion. In neutrocclusion, the molar and canine relationships are Class I and the overjet is normal. In distocclusion, the molar and canine relationships are Class II and the overjet is either greater than normal (Division 1) or normal (Division 2). In mesiocclusion, the molar and canine relationships are Class III and the overjet is smaller than normal, usually negative.
Distocclusion can occur in many different configurations:
- Backward-positioned mandible with a normally positioned maxilla
- Backward mandible with a forward maxilla
- Backward mandible with a less backward maxilla
- Normal mandible with forward maxilla
- Forward mandible with more forward maxilla
Thus, the finding of mesiocclusion or distocclusion reveals a discrepancy in jaw position between the upper and lower jaws, and cannot be used independently to determine anteroposterior jaw position. Also note that the finding of neutrocclusion does not necessarily imply normal anteroposterior jaw position, as both jaws can be retrognathic or prognathic.
To complete the assessment of anteroposterior jaw position, one also evaluates the facial profile.13-16 Traditionally, clinicians have assessed the profile by classifying it into one of three categories: straight, convex, or concave. However, this assessment lacks specificity. For example, a concave profile can occur when the upper jaw is normal and the lower jaw is prognathic, when the upper jaw is retrognathic and the lower jaw is normal, or when the upper jaw is retrognathic and the lower jaw is prognathic.
A better method is to compare the anteroposterior position of each jaw with the anterior boundary of the cranial base. Three structures related to the anterior cranial base—soft-tissue glabella, soft-tissue nasion, and the most anterior aspect of the cornea—have been successfully employed to define the anteroposterior position of a coronal plane of reference.
When assessing the facial profile, the patient should be in standard anatomical alignment (i.e., head in the NHP), with the clinician observing from the side. While in this position, the clinician imagines a coronal plane of reference—a plane that can be tangential to soft-tissue glabella, soft-tissue nasion, or the anterior surface of the cornea. Concurrently, the clinician infers the anteroposterior position of the jaws by assessing the position of the lips and chin in relation to this paracoronal plane (Figure 5).
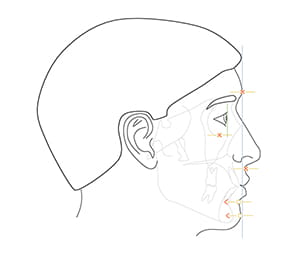
Figure 5
No perfect reference plane exists for determining the anteroposterior position of the jaws. Nasion can be obscured in Asian patients, as it is commonly located posterior to the cornea; glabella can be distorted in frontal bossing; and distances from the cornea are difficult to gauge clinically. Notwithstanding these limitations, our clinical impressions are reliable because our brains have the innate ability to discern the correct anteroposterior position.
Vertical
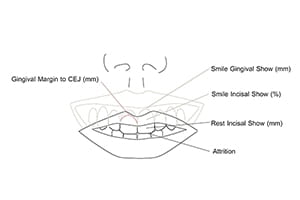
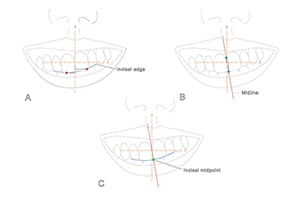
Clinically, one determines the vertical position of the maxilla by measuring the rest-incisal-show and the smile-dento-gingival-show (Figure 6). Rest-incisal-show is the amount of upper incisor that is exposed when the lips are relaxed. It is the vertical distance from the upper lip stomion to the maxillary incisal midpoint. Stomion is the midpoint of the free-edge of a lip, upper or lower. The incisal midpoint is the point at the intersection of the dental midline and the arc defined by the incisal edges (Figure 7). It represents the middle of the dental arch. When the maxillary incisal midpoint is below stomion (baseline), the rest-incisal-show is positive; when above, it is negative. Rest-incisal-show should be measured at the incisal midpoint rather than at other points on the incisal edges because, when the maxilla is canted, incisal show varies at each location (Figure 7).
Rest-incisal-show should be measured on an upright patient, as it can increase when the patient is supine (Figure 8). Additionally, the eyes of the examiner should be level with the patient’s lips, as looking from above hides the teeth, and viewing from below exposes them. Negative incisal shows are difficult to measure. To overcome this challenge, the authors place a piece of wax on the lingual surfaces of the upper incisors, extending it downward below the lip. Subsequently, the clinician asks the patient to relax his lips and marks (on the wax) the position of the upper lip stomion. Finally, the clinician pulls the upper lip up and, with a caliper, measures the distance from the mark to the incisal midpoint (Figure 9). Some patients may have incisal attrition, which is the erosion of the incisal edges due to grinding. In this situation, the examiner should add the amount of tissue loss to the measurement.
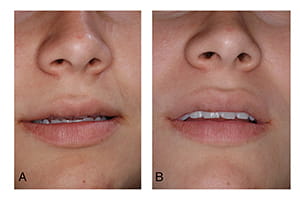
Figure 8
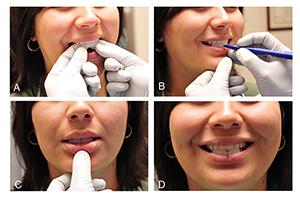
Figure 9
To determine the vertical position of the maxilla, the examiner compares the patient’s rest-incisal-show with normal values. Gender, age, ethnicity, and the length of the upper lip influence these values.17 Female patients have more incisal show than males. Incisal show also decreases with age.17, 18 Caucasians tend to have more incisal show than patients of other ethnicities.17 Patients with short upper lips tend to have more incisal show than those with longer lips.17 For example, a five-millimeter incisal show is considered normal in a teenage girl with a short upper lip, while a one-half millimeter incisal show is considered normal in a 60-year-old male. Patients with a negative incisal show are deemed to have deficient maxillary downward displacement, and patients with incisal shows above the normal range for their particular gender, age, ethnicity, and length of upper lip are deemed to have excessive maxillary downward displacement.
As stated previously, smile-dento-gingival-show is also used to determine the vertical position of the maxilla. Smile-dento-gingival-show is the amount of central incisor and labial gingiva displayed when smiling. Tooth show is measured as a percent of its height, while gingival show is measured in millimeters. While smiling, most patients with normal vertical maxillary position display 100% of their incisors19 and up to 2 mm of gum. Patients with superiorly positioned maxillae show less than 100% of their incisors, whereas patients with inferiorly positioned maxillae display an excessive amount of gum.20 Yet the amount of tooth and gum displayed during the process of smiling is not only related to the vertical position of the maxilla, it is also associated with lip animation and passive dental eruption.
Too much or too little tooth and gum displayed during smiling may be a consequence of abnormal lip animation.21, 22 A hyperactive smile—caused by hyperactive smile muscles—produces a “gummy” smile; a hypoactive or weak smile, results in significantly less tooth display. Hyperactive smile is diagnosed when the gingival-show is large, the rest-incisal-show is normal, and passive dental eruption (next paragraph) is normal. A hypoactive smile is diagnosed when the smile-tooth-display is small and the rest-incisal-show is normal.
Tooth eruption can consist of active and passive phases. Active eruption is the movement of teeth toward the occlusal plane, while passive eruption is related to the exposure of teeth through apical migration of the gingiva. When passive eruption does not progress, the result is a dental crown that appears short because of the presence of excess gingiva covering the enamel. Clinically, the most obvious sign of delayed passive eruption is a short clinical crown; also, sulcus depths, from the gingival margin to the cement-enamel-junction, are large (over 3 mm).1
Patients with delayed passive eruption may have large smile-gingival-shows, despite normal vertical maxillary position. In this scenario, the smile-gingival-show is large, but the rest-incisal-show is small or normal.
Transverse
Clinically, transverse jaw position is established by measuring the distance between middle landmarks and the median plane. In the maxilla, one solely measures the position of the upper incisal midpoint. In the mandible, however, one measures the position of two points: the lower incisal midpoint and soft-tissue pogonion (i.e., the most prominent point of the soft-tissue chin). The transverse position should be measured at the incisal midpoint points rather than any other point on the dental midline because when the jaws are canted, measurements vary with point position (Figure 7). Also, when assessing the transverse position of the mandible, the mandible must be in centric relationship—the mandibular position in which the condyles are fully seated within the glenoid fossae.
Table of Contents
